MLS – PSYCHOLOGY RESEARCH (MLSPR)https://www.mlsjournals.com/ISSN: 2605-5295 |

|
(2025) MLS-Psychology Research, 8(1), 91-107. doi.org/10.33000/mlspr.v8i1.4174
Risk factors for emotional overload in unpaid caregivers of dependent and disabled people
Rodrigo A. Cárcamo
San Sebastian University (Chile)
rodrigo.carcamol@uss.cl · https://orcid.org/0000-0002-1825-0097
Alejandro Yelincic
International Iberoamerican University (México)
ayelincic@rehabilitamos.org · https://orcid.org/0000-0002-1825-0097
Abstract: In Chile, an important part of the population requires care due to their level of disability and/or dependence. The main caregivers experience emotional overload, negatively affecting their quality of life. The aim of this study was to identify psychosocial risk factors of overload in caregivers of dependent and disabled people.. The study design is non-experimental, cross-sectional, ex-post simple retrospective, causal-correlational. Data from 2,093 caregivers attending the Corporación de Rehabilitación Club de Leones Cruz del Sur, Chile, were analyzed. A total of 2,093 caregivers of people with disabilities and/or dependence who met the inclusion criteria were included and answered questions about sociodemographic information and the Zarit caregiver overload scale. The results show that caregiver age, caregiver sex, family structure and dependent's age group were significant predictors of caregiver emotional overload measured with the Zarit scale. The present study identified that the psychosocial variables that are related to overload are that the caregivers are women, that the older the caregivers are, the greater the risk of presenting overload, that they are part of single-parent families and that they take care of adults or older adults; to the extent that these variables are present, there is a greater risk of presenting emotional and/or physical overload.
Keywords: Dependency, caregiver overload, primary caregiver, disability.
Factores de riesgo de la sobrecarga emocional en personas cuidadoras no remunerados de personas en situación de dependencia y discapacidad
Resumen: En Chile, parte importante de su población requiere de cuidados debido a su nivel de discapacidad y/o dependencia. Las personas cuidadoras principales, experimentan sobrecarga emocional, afectando negativamente su calidad de vida. Este estudio tuvo por objetivo identificar factores psicosociales de riesgo de sobrecarga en cuidadores de personas en situación de dependencia y discapacidad. El diseño del estudio es no experimental, transversal, ex – post – factos retrospectivos simples, de carácter causal-correlacional. Se analizaron 2,093 cuidadores de personas en situación de discapacidad y/o dependencia que cumplían con los criterios de inclusión, quienes respondieron preguntas sobre información sociodemográfica y la escala de sobrecarga del cuidador Zarit que asisten a la Corporación de Rehabilitación Club de Leones Cruz del Sur, Chile. Los resultados muestran que la edad del cuidador, el sexo del cuidador, la estructura familiar y el grupo etario del dependiente fueron predictores significativos de la sobrecarga emocional de los cuidadores medidas con la escala Zarit. El presente estudio identificó que las variables psicosociales que se relacionan con la sobrecarga; es que sean cuidadoras mujeres, que a mayor edad de las cuidadoras mayor riesgo de presentar sobrecarga, que integren familias de tipo monomarentales y que cuiden adultos o adultos mayores, en la medida que estas variables estén presentes, existe mayor riesgo de presentar sobrecarga emocional y/o física.
Palabras clave: Dependencia, sobrecarga de la persona cuidadora, persona cuidadora no remunerada, discapacidad.
Introduction
In Chile, about 18% of the adult population and 15% of the child and adolescent population have some degree of disability (Ministry of Social Development and Family, 2023a, 2023b). Likewise, 9.8% of the country's adult population is in a situation of dependency (Ministry of Social Development and Family, 2023c). Some estimates indicate that by 2050, the population pyramid will be inverted and historical percentages of people over the age of 80 will be reached (Instituto Nacional de Estadísticas, 2018), which implies a higher probability of people in a situation of disability and/or dependence in Chile.
Chile is very close to reaching indicators comparable to those of countries such as Japan or Sweden, where it has one of the highest life expectancies in the world (National Institute of Statistics, 2025). This demographic change requires the design and implementation of public policies that comprehensively address the emerging needs associated with population aging, including the care of dependent persons.
A significant proportion of this care falls on so-called unpaid primary caregivers, who are usually immediate family members who assume this responsibility without professional support or financial remuneration. Several studies have shown that this group faces high levels of physical and emotional burden, resulting in conditions such as musculoskeletal pain, chronic fatigue, social isolation, affective disorders, and symptoms of anxiety and depression (Lillo-Crespo et al., 2018; Schulz & Eden, 2016).
These impairments in the caregiver's health can have negative side effects on the quality of care provided to the dependent person. It has been documented that elevated levels of caregiver overload and stress may be associated with increased risk of neglect, abuse (verbal or physical), and even caregiving neglect (Dong, 2015). In turn, these situations profoundly affect the family environment, generating tensions, conflicts and dysfunctions that compromise the psychological well-being of all family members (Pinquart & Sörensen, 2003).
Therefore, it is urgent to advance in the generation of support systems for unpaid caregivers, including training, psychosocial support, respite networks and institutional recognition of their role, with the aim of safeguarding both their well-being and that of the people under their care.
The role of the unpaid primary caregiver of people with dependency and/or disability in this current scenario is therefore crucial. Caregivers take care of the basic needs and particular treatments required (cognitive stimulation, physical exercises, pharmacological treatments, among others) to improve the quality of life of dependent persons. This involves changes in the caregiver's daily routine that have an impact at the economic, health and family level (Bauer & Sousa-Poza, 2015), such as reduced hours of paid work, lower pay, health affectation, decreased quality of family life. Along with this, primary caregivers generally fulfill this role alone (Kahriman & Zaybak, 2015) and with little or no financial support from the state. This context generates pressure on caregivers that can lead to a psychological state called caregiver emotional overload, which involves the perception of feeling overwhelmed or overwhelmed on a physical and psychological level as a result of the tasks they perform (Silva et al., 2021). It is estimated that about 30% of caregivers present moderate to high levels of emotional overload (Gérain & Zech, 2021; Ilse et al., 2008) that are expressed in emotional problems such as isolation, overwhelm, exhaustion and chronic stress (Brummett et al., 2006; Domínguez et al., 2012; Flores et al., 2015).
In Chile there is a system of care for children and adults, but its presence in public policies is unclear and confusing for the community. Children and adolescents with disabilities or dependency often spend years in a special education system that provides them with both training and specific care.
Although progress has been made in policies for children and adolescents, there is a significant gap with respect to those aimed at adults with dependency. To address this, Chile has initiated a National Care Plan that includes a census of caregivers and the creation of long-stay facilities for the elderly in each commune, offering specialized care for people with loss of autonomy.
Local governments may develop strategies to support families with dependents, but they generally focus only on health services, without comprehensively addressing the various dimensions of care.
The main unpaid caregivers of people with disabilities and dependency perform a rather silent role, that is to say, they are not usually the focus of attention in the midst of this problem and are distanced from public policies as recipients of aid or benefits, subjecting themselves day after day to levels of emotional overload.
According to studies in Latin America, Montoya et al. (2018) in Colombia, found that the average age of caregivers is 46 years and that the majority are women (74%), with the kinship relationship being the most prevalent (36%), followed by spouse (26%), in addition, 66% do not have higher education, with 95% of caregivers presenting a certain degree of emotional overload, especially in those who did not present family support networks or public services.
So far, little is known about caregivers of people with disabilities and/or dependence in our country, and it is of utmost importance to know the psychosocial characteristics that may interfere in this role. According to a study conducted in Chile, most of the people who need support in caregiving receive it from their relatives, according to Yelincic and Cárcamo (2021), mainly female caregivers, reaching 84.9% of the total number of caregivers in the sample of this study (n = 936), and this role that falls on women increases when it comes to caring for dependent children (91.8%). In general, these caregivers do not have the knowledge or training to attend to the needs of the dependent person. In addition, this same study indicates that the caregivers of children are mostly mothers, and in the case of adults and older adults it is their partners and, in second place, mothers and daughters, respectively.
Another finding of this study was that physical disabilities are the main reason for having a primary caregiver. The diagnoses are associated with diseases of the Central Nervous System and/or amputations, with cerebrovascular diseases being determinant in the groups of adults and older adults, compared to children who are more associated with diseases related to cerebral palsy (Yelincic & Cárcamo, 2021). In general, adults and older adults experience disability as the loss or deterioration of certain motor or cognitive skills, whereas in the case of children who suffer the experience of disability, their families generally experience a different process with their children, where the absence of motor and/or cognitive skills accompanies them from birth. The psychosocial intervention processes are different, although in both there is an adjustment or a family reorganization of the functions and roles within the home, however, in the adult and older adult, the family must adapt to a loss of an acquired skill, having to adjust to the new characteristics and demands of the family member.
Espinoza and Aravena (2012) in a descriptive study in Chile reported that 90% of caregivers were women between 37 and 86 years of age (M = 57.0). In terms of schooling, only 3.3% of the caregivers had higher education, and the majority of caregivers are cared for by their mother, secondly by their spouse, and thirdly by a sibling. This study also showed that 63% of the caregivers had a permanent illness and most of the caregivers had mild caregiver strain with little perceived social support.
Also in Chile, Lavoz et al. (2009), found that the main caregivers of dependent persons were women (79%), between 20 and 50 years of age, with low schooling and that the majority were daughters who take care of their parents. In relation to overload, 20% presented mild overload and 38% presented intense overload.
Zepeda-Alvarez and Muñoz-Mendoza (2019), studied 43 caregivers of older adults in Chile, and note that 69.77% presented overload. In addition, the majority of unpaid caregivers are women (74.42%), who assume this role because it is socially acquired and that only men can assume this role in the absence of women in their close family group. At the educational level, 13.95% have higher education and it is mainly the daughters of dependent parents who are involved in caregiving, followed by the spouses of dependent persons.
All of the above demonstrates the existence of a global social problem, whose reality is expanding and is recognized transversally, where a large part of the world is experiencing an aging of its population, which brings with it new challenges in the trajectory of life and will require a reorganization of the family system. When this occurs, a need for care is identified and, consequently, a person is identified who is able to exercise the role of primary caregiver for the partially or totally dependent person.
According to Arriagada (2010), there is a social organization of care (OSC) composed of social, political and economic interrelationships. The author clarifies that caring is the satisfaction of the physical and biological needs of another, in a period of their life cycle, and that this triad can be exercised from the domestic sphere, considering here unpaid caregivers, women with emotional ties; or from the contractual sphere, in which are found paid caregivers, mainly household advisors; and, finally, from specialized medical services, which are often costly for the family group.
Emotional overload of the caregiver not only has a huge impact on the caregiver's quality of life, but also has harmful effects on the dependent. Several studies have shown a relationship between caregiver emotional exhaustion and likelihood of physical and emotional abuse (Johannesen & LoGiudice, 2013) and neglect (Andela et al., 2021).
The assumption of the role of caregiver usually occurs suddenly and unplanned, emerging as an immediate response to the appearance of a need within the family nucleus. Unlike caregiving in childhood -a stage in which the birth of a new member implies a social and biological expectation regarding the caregiving role, traditionally assigned to mothers-, the onset of a disability or dependency situation in adulthood or old age is not usually accompanied by prior preparation or formally defined support structures (Arriagada, 2020; Lillo-Crespo et al., 2018). While in childhood dependency is anticipated and normatively accepted as part of human development, in adulthood or old age the need for care generates a forced reorganization of the family environment, often without adequate state support or sufficient community networks (Durán & Rogero-García, 2009). This response, usually spontaneous and without prior training, involves the abrupt incorporation of a complex role-that of informal or unpaid caregiver-for which most people have not been prepared, posing challenges at both the individual and systemic levels (Schulz & Eden, 2016).
It is there where the existence of gender, economic, family or other components become evident, falling naturally on one person in the family group, which is usually someone of the female gender. Thus, it is considered necessary to visualize the risk factors in those caregivers who will begin this work in order to help them before they begin to feel emotional and/or physical discomfort as a result of the overload of caring for a dependent.
From an early age, men and women learn about what it means to be a man or a woman, even though there is a second cycle of defining sexual and gender identity during puberty. As Ovejero (2013) says "it is gender identity that "forces" men and women to be, to think, to feel and to behave". The primary socializing components such as the family and the media help in the role adjustment of men and women.
Gender stereotypes tend to exalt the masculine as synonymous with power and autonomy, which contributes to the devaluation of the feminine. Gender identity, traditionally associated with roles such as mothers and wives, has begun to transform towards more autonomous and personal development-oriented models (García & Navarro, 2016). The female body, historically linked to motherhood and the domestic sphere, has been a factor of exclusion in productive spaces.
The feminization and inequity of care work leads to a profile associated with unemployed women, with low schooling, responsible for housework, where there is a moral commitment, marked by affection, responsibility, an imposed task, not valued or remunerated, while the male gender is only given the option of assuming housework, which includes care work (García-Calvente et al., 2004)
On the other hand, language reinforces these inequalities by identifying women according to their marital status or family role, while men are associated with their profession (West, Lazar & Kramarae, 2001). From a social perspective, gender is historically constructed and reconstructed through language, culture and norms (Lamas, 1996; Scott, 2000), which allows us to rethink the categories of "man" and "woman" beyond biological determinism (García & Navarro, 2016).
A central tenet of feminist analysis is that care work, especially informal care work, falls disproportionately on women, reflecting and perpetuating patriarchal structures and gender divisions in society (Petrie-Flom Center, 2021). This work is often unpaid, undervalued or underpaid, which is a fundamental concern in feminist political economy, which denounces the invisibilization and lack of social recognition of these essential tasks for social and economic sustainability (Folbre, 2021). On the other hand, the intersectionality approach, coined by Kimberlé Crenshaw (cited in Bond Disability and Development Group, 2024), allows us to understand how multiple social identities-including race, gender, social class, age, sexual orientation, caste, and migratory status-intersect to shape complex experiences of discrimination and marginalization. In this sense, disability should not be conceived in isolation, but as an experience that is intertwined with other aspects of identity, affecting inclusion and access to rights at multiple levels.
Stereotypes are culturally constructed and shared by a significant number of societies, and it is possible to affirm that in many of them, care work is part of women's gender identity, in a predictable manner, since societies tend to guide our roles in how we should be and how we should behave, and therefore, dedicating oneself to housework or having more competencies in care work constitutes an attribute that socially differentiates them from men, who are expected to perform roles that are mostly associated with being the economic provider of the household.
The physical and/or emotional overload experienced by caregivers of dependent or disabled persons is a phenomenon of high clinical and social relevance, with direct implications on their overall health. This overload can manifest itself at the physical level, through musculoskeletal symptomatology associated with inadequate postures during mobilizations or transfers of the patient, as well as through somatizations derived from chronic exhaustion (Lillo-Crespo, Riquelme, & Sánchez, 2018; Pinquart & Sörensen, 2003). However, the impact is not limited to the physical plane, but is often expressed in the emotional realm as well, or even in the confluence of both domains. On the psychoemotional level, it is common to observe increased levels of irritability, persistent feelings of exhaustion and stress, as well as the appearance of social withdrawal behaviors, attributable to the cumulative wear and tear of the caregiving task (Schulz & Eden, 2016; Zarit, Reever, & Bach-Peterson, 1980). Likewise, sleep disturbances, loss of appetite, decreased self-esteem and flattened affectivity have been identified, factors that, together, could be relevant predictors for the development of mood disorders, particularly depression, in the medium or long term (Vitaliano, Zhang, & Scanlan, 2003).
The physical and/or emotional overload of caregivers of people with dependency and disability, brings consequences in the caregiver, as he/she begins to present physical pain, product of the inadequate postures in the transfers of the dependent or somatize ailments due to fatigue or overwhelm that he/she presents as a result of caring for a third party. Not only physical pain is present, but many times it is presented from the emotions, and even both can be present. From the emotional point of view, we find that the main caregivers are more irritable, they express feeling exhausted and stressed, they tend to show behaviors such as social isolation due to listlessness and daily wear and tear, they show greater affective apathy which affects their relationship with others, they have problems sleeping, loss of appetite, low self-esteem and other situations that could be configured in the future as factors conducive to the development of depression.
Associated with the above, the relationship between the caregiver and dependent may be threatened because there may begin to be conflict between them, which could trigger aggressive behavior on the part of the caregiver as well as the belief on the part of the dependent that his relative or dependant only seeks other interests from him, or a significant emotional discomfort that also needs the support of a third party that can resolve clinical pictures of possible depression or some other more serious emotional disturbance.
Based on this background, it is considered relevant to investigate the characteristics of unpaid caregivers of dependent persons, due to the impact this role has on mental health, not only on the caregiver, but also on those he/she cares for. The identification of variables associated with the risk of emotional overload can promote psychological and social interventions to avoid increasing mental health problems in a group with particular characteristics, in a society with an increasing population of elderly people who require care when compromising their autonomy and independence.
The objective of this study is to identify risk factors for the presence of emotional overload in the unpaid caregiver of dependent persons. It is hypothesized that those with the greatest emotional overload are female caregivers, who care for adults and older adults and who belong to a family with few support networks, as measured by the single-parent structure of the family.
Method
This is a non-experimental, cross-sectional, ex-post simple retrospective, quantitative, causal-correlational research, which aims to distinguish the psychosocial risks of unpaid primary caregivers of people in a situation of dependency, who attend the Corporación de Rehabilitación Club de Leones Cruz del Sur in the Region of Magallanes and Chilean Antarctica, Chile.
The data were extracted from the institution's electronic clinical records, which contain the social survey and the application of the Zarit scale. The participants were caregivers of children, adults and older adults of people who present dependency associated with a diagnosis of disability.
Data were grouped according to the variables of primary caregiver overload and no primary caregiver overload. Once the data had been standardized, correlation analyses of the different variables and group comparison analyses were performed. In order to identify the variables that explain the variance of emotional overload, logistic regressions were used, since the variable overload was treated as a categorical variable.
Sample
The type of sample was non-probabilistic, by convenience. Secondary analyses were performed on the database of N = 2,093 unpaid caregivers of patients with disabilities at the Corporación de Rehabilitación Club de Leones Cruz del Sur (CRCLCS) in the Region of Magallanes and Chilean Antarctica, Chile. The average age of caregivers was 36 years (M = 36.21, SD = 11.39), M = 33.09 for those caring for children, M = 51.04 for those caring for adults, and M = 54.83 for those caring for older adults (see Table 1).
Unpaid caregivers of dependent and disabled users were selected for this study. We included primary caregivers of CRCLCS users who: a) spend most of their time prostrate and/or with significant difficulty getting around or b) who, because of their physical, sensory and/or cognitive disability, require a third party to assist them. Other inclusion criteria were admission to CRCLCS between 01-01-2018 and 10-10-2021 and that caregivers had answered the interest questionnaires voluntarily. Paid caregivers and/or caregivers of institutionalized patients were excluded.
Instruments
The data collection was carried out by teams of professionals belonging to the psychosocial and medical areas of the CRCLS as a protocol for the admission of the users of the institution. Through an interview and assessment, sociodemographic information was collected from caregivers and/or patients, such as economic income, level of schooling, age, sex, marital status, kinship, housing conditions, diagnosis, among others. In addition, caregivers responded to the Zarit caregiver overload scale (Breinbauer et al., 2009). This instrument has been validated for the Chilean population and consists of 22 questions that ask about the perceived impact on the caregiver's life due to caregiving. It is answered on a 5-point Likert-type frequency scale (1 = never to 5 = almost always), where higher scores indicate higher levels of caregiver overload.
For the vulnerability bracket, in Chile the population is divided into seven vulnerability brackets; the first between 0% to 40% of lower income; second between 41% to 50% of lower income; third 51% to 60% of lower income; fourth between 61% and 70% of lower income; fifth between 71% and 80% of higher income; sixth between 81% and 90% of higher income; and seventh between 91% and 100% of higher income.
This study was approved by the ethics committee of the Universidad Internacional Iberoamericana, in its session of February 11, 2022 and complies with the ethical code of the World Health Organization on human studies.
Results
According to the descriptive analysis of the total sample, it can be observed that a large majority of the caregivers are women (92.20%), on the contrary, the patients are mostly men (63.20%). Most of these families had a two-parent family structure (65.70%) and did not belong to the most vulnerable 40% of the population (58.60%). On the other hand, caregivers caregivers were mostly represented at the intermediate educational level (58.10%). All variables separated by age group to which the patient belongs are reported in the table below (Table 1).
Table 1
Descriptive statistics of the sample (N = 2,093)
|
Variables |
Child | Adult | Senior Citizen | Total | |
|
X̄(SD) o % X̄(SD) o % X̄(SD) o % X̄(SD) |
X̄ (SD) or |
X̄ (SD) or |
X̄ (SD) or |
||
| Age of caregiver |
33.09 (7.46) |
51.04 (13.18) |
54.83 (13.60) |
36.21 (11.39) |
|
| Sex of caregiver (female) |
94.20 |
76.50 |
82.70 |
92.20 |
|
| Sex of patient (female) |
36.10 |
36.70 |
43.20 |
36.80 |
|
| Educational level of the caregiver | |||||
| Under |
7.10 |
30.60 |
33.20 |
10.90 |
|
| Medium |
59.80 |
55.10 |
45.50 |
58.10 |
|
| High |
33.10 |
14.30 |
21.40 |
31.00 |
|
| Vulnerability section (si)b |
43.60 |
34.70 |
26.80 |
41.40 |
|
| Family types | |||||
| Single-parent |
29.90 |
36.70 |
41.80 |
31.50 |
|
| Biparental |
69.40 |
57.10 |
40.50 |
65.70 |
|
| Others |
0.70 |
6.10 |
17.70 |
2.80 |
|
| Caregiver overload |
41.15 (11.65) |
50.15 (14.55) |
49.66 (15.34) |
41.47 (12.62) |
|
Note. aAge in years; b0= Does not belong to the most vulnerable 40%, 1= Does belong to the most vulnerable 40%. Nchild = 1775, Nadult = 98, Nolder adult = 220.
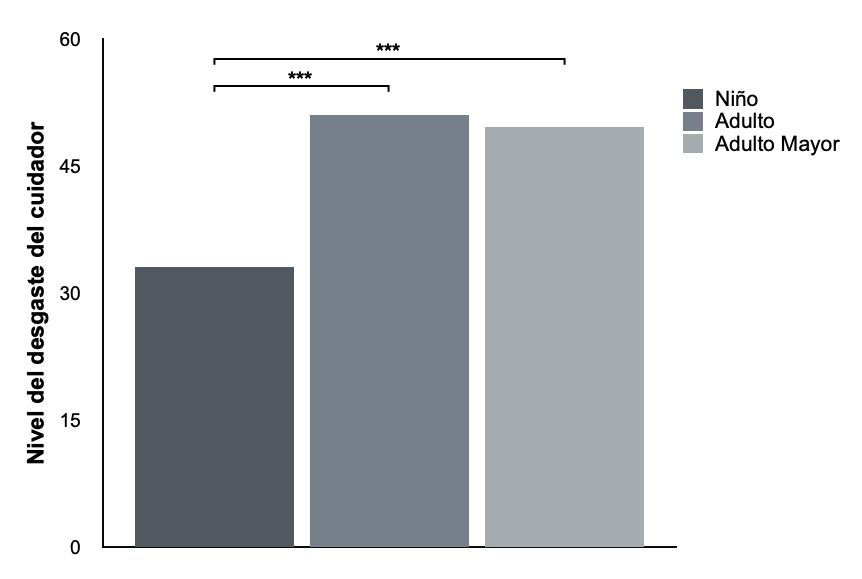
A one-way ANOVA analysis of variance was performed to determine whether the level of caregiver attrition caregivers age group to which the cared-for patient belongs (See Figure 1). Significant differences were found in the level of attrition between groups (F (2, 2090) = 67.60, p < .001; ηp² = .06). Posthoc analysis showed that adult caregivers had a higher level of burnout (M = 50.15, SD = 14.55) than child caregivers (M = 41.15, SD = 11.65; p < .001). Similarly, caregivers of older adults (M = 49.66; DE = 15.34) were found to have a significantly higher level of burnout than caregivers of children (M = 41.15, DE = 11.65; p < .001). No significant differences were found between the level of burnout of adult and older adult caregivers (p > .05). (figure 1)
Figure 1
Level of caregiver overload according to the age group to which the patient belongs (N = 2,093).
Two-way ANOVAs were performed independently to determine the effect of patient age group and other demographic characteristics (patient and caregiver sex, caregiver educational level, vulnerability band and family type) on caregiver burnout. In all models, only the main effect of the age group to which the caregiver belongs was significant.
A bivariate correlation analysis was performed to determine the degree of association between the variables of interest. As seen in Table 2, a positive correlation was found between caregiver burnout level and caregiver age (r = .21, p < .001), caring for adults compared to children (r = .14, p < .001), caring for older adults compared to children (r = .20, p < .001), and having a single-parent (r = .08, p < .001), and other type of family (r = .08, p < .001) compared to a two-parent structure. On the other hand, a negative relationship was found between caregiver emotional exhaustion and belonging to the 40% vulnerability bracket (r = -.05, p < .05), which means that those who belong to the vulnerability bracket present less emotional exhaustion than those who do not belong to that bracket. (table 2)
Table 2
Correlation between sociodemographic variables and the level of caregiver overload (N = 2,093)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| 1. Age of caregiver |
- |
|
|
|
|
|
|
|
|
| 2. Sex of caregivera |
.20*** |
- |
|
|
|
|
|
|
|
| 3. Sex of patienta |
.02 |
-.05* |
- |
|
|
|
|
|
|
| 4. Age group (adult)b |
.29*** |
13*** |
.00 |
- |
|
|
|
|
|
| 5. Age group (older adults)b |
.56*** |
.12*** |
-.05* |
-.08*** |
- |
|
|
|
|
| 6. Educational level of P. caregiverc |
-.27*** |
-.05* |
.01 |
-.13** |
-.18*** |
- |
|
|
|
| 7. Vulnerability sectiond |
-.02 |
.00 |
-.00 |
-.03 |
-.10*** |
.28*** |
- |
|
|
| 8. Type of family (single-parent)e |
.02 |
-.05* |
-.02 |
.02 |
.08*** |
-.05* |
-.12*** |
- |
|
| 9. Type of family (other)e |
.25*** |
.03 |
.01 |
.05* |
.31** |
-.11*** |
-.08*** |
-.11*** |
- |
| 10. Level of caregiver overload |
.21*** |
-.011 |
.02 |
.14*** |
.20*** |
-.04 |
-.05* |
.08*** |
.08*** |
Note. *p < .05 **p < .01, ***p < .001
a0 = female, 1 = male; bCompared to age group of child patients; c0 = low, 1 = medium, 2 = high; d0 = does not belong to 40% most vulnerable, 1 = belongs to 40% most vulnerable; eCompared to two-parent family type.
To determine the effect of sociodemographic variables on caregiver burnout, a multiple regression analysis was performed (see Table 3). The independent variables were the age of the caregiver, the sex of the patient and caregiver, the age group to which the patient belongs, the educational level of the caregiver, the family vulnerability level and the type of family. Caregiver burnout was entered as an independent variable. The variable selection method was a one-step input method and the listwise elimination method was used to handle missing data.
Results indicated that the model was significant (F(9, 2083) = 18.73, p < .001), explaining 8% of the variability in caregiver burnout (R2 = .08, p < .001). Caregiver age (β = .11, t(2083) 3.67 , p < .001) significantly predicted caregiver burnout, indicating that greater caregiver burnout occurs with greater age. On the other hand, the sex of the caregiver was also a significant predictor (β = -.06, t(2083) -2.82 , p < .01), with female caregivers presenting higher levels of burnout. Considering the age group of patients, caring for adults (β = .13, t(2083) 5.44 , p < .001) and caring for older adults (β = .15, t(2083) 5.43 , p < .001) were found to be significantly more wearing than caring for children. Finally, the results showed that belonging to a single-parent family predicted a higher level of caregiver burnout than being in a two-parent family (β = .06, t(2083) 2.62 , p < .01). (table3)
Table 3
Multiple regression of sociodemographic variables on caregiver strain (N = 2,093)
| Variable | B | SE B | β | |
| Age of caregiver | .12 | .03 | .11*** | |
| Sex of caregivera | 2.87 | 1.02 | -.06** | |
| Sex of patienta | .63 | .55 | .02 | |
| Age group (adult)b | 7.57 | 1.39 | .13*** | |
| Age group (older adults)b | 6.19 | 1.14 | .15*** | |
| Educational level of the caregiverc | .91 | .47 | .04 | |
| Vulnerability sectiond | -.74 | .57 | -.03 | |
| Type of family (single-parent)e | 1.54 | .59 | .06** | |
| Type of family (other)e | 1.09 | 1.74 | .01 | |
| R2 | .08*** | |||
| F | 18.71*** |
Note. **p < .01, ***p < .001
a0= female, 1 = male; bComparison with age group of child patients; c0 = low, 1 = medium, 2 = high; d0 = does not belong to the most vulnerable 40%, 1 = belongs to the most vulnerable 40%; eComparison with the type of two-parent family.
Discussion and Conclusions
The present study identified four psychosocial factors related to increased caregiver burnout. First, when this function is expressed in the advanced age of the caregiver (post parental), it is a crisis that triggers an increased risk of overload. Second, being a female caregiver was found to increase the likelihood of emotional overload. As mentioned in both Chilean and foreign studies, it is mainly women who are in charge of the caregiving role. This, being linked to gender expectations or mandates, such as, for example, that women have greater caregiving skills than men, is related to low valuation of this work and less support from other family members.
Third, it was found that caregivers caring for adults or older adults were more overburdened than caregivers caring for children. This result is similar to that found by Escandell-Rico and Pérez-Fernández (2022), who point out that older caregivers are more at risk of overload. This can be explained, on the one hand, by the relationship that has been found in the literature between age and the probability of presenting high levels of dependence. Greater dependency, therefore, requires more caregiving tasks and less free time to perform other tasks that allow them to detach from the role on a daily basis, making emotional overload more likely. On the other hand, since the caregiving role is generally assumed by older adult partners, there are more barriers to performing the tasks (wear and tear, old age, less energy, illness, etc.). In addition, our own results indicate that caregivers of older adults present high levels of vulnerability, which is a chronic stressor within the family context. Finally, it is possible that for caregivers of children with disabilities, there are more internal and external support networks (e.g., school), which are lost in adulthood.
Finally, belonging to a single-parent family was found to be related to higher levels of caregiver burnout. A family group with more adults in the household can divide certain roles, which facilitates the task of caregiving. In general, these families are often made up of several people who can act as caregivers, alternating functions and also making possible the presence of actions other than caregiving; some may work partially or include self-care activities in their weekly routines, which means less emotional and/or physical wear and tear or overload.
Contrary to other research, educational level was not found to be a significant predictor of caregiver overload. The support networks at the family or public service level that an unpaid primary caregiver possesses would then be more relevant, since caregiving is especially a task that is learned from the virtue of practice and initial child rearing, being transmitted from generation to generation.
The present research provides relevant data that allow the identification of risk variables for caregiver emotional exhaustion, being the age and gender of the caregiver, the age group of the dependent person and the family structure, thus allowing the possibility of constructing a psychosocial risk pattern that may anticipate the psychosocial teams of a possible risk of overload in an unpaid primary caregiver.
Unpaid primary caregivers of people with disabilities and dependency worldwide are an issue that emerges as a challenge for most societies, at least in the Western world, where many of our expectations about caregiving and caregivers are culturally shared, at a time when the proportion of older adults is increasing. (Economic Commission for Latin America and the Caribbean, 2022).
Currently, it can be seen that, in the work of caring for others, the male figure is not present in a significant way, but only appears in the absence of the female gender. With this it can be inferred that the competencies to perform this function are not necessarily related to physiological issues, but rather, to the cultural determination and expectations that exist in a society, where women are "better" at performing these functions compared to men. The cultural reasons for the construction of this stereotype is that from an early age they begin to differentiate roles within the family (Arriagada, 2010), therefore, it is expected for many that this work is performed by women. When this social group of primary caregivers perceive themselves in the same social category and/or present a common social identification (Sanchez & Gonzalez, 2012), they begin to feel that it is part of their role. Unpaid primary caregivers of people with disabilities and dependency begin to be seen as a stereotyped social category, where they share roles and attributes, forming a group marked by actions related to caring for another.
There is no doubt that, according to different theorists, the construction of roles is a cultural issue and that this can be transformed with incentives that allow the male gender to identify not only productive but also part of the solution to care, understanding that the development of societies is achieved when all actors take charge of the problems existing in a territory (Economic Commission for Latin America and the Caribbean, 2022).
Main Conclusions
Understanding gender as a social construct, influenced by stereotypes, traditional roles, language and socialization processes since childhood (García & Navarro, 2016; Ovejero, 2013), allows for a deeper analysis of the emotional overload faced by unpaid caregivers. These tasks continue to be assumed, for the most part, by women, reflecting an unequal distribution of care responsibilities based on gender mandates. This situation contributes to the physical and emotional exhaustion of those who perform caregiving tasks on a constant basis and without formal recognition.
In this context, elderly caregivers and those who belong to single-parent families are at high risk of emotional overload, especially when they do not have support networks. In addition, it is observed that caring for adults or elderly people entails higher levels of emotional demands than caring for children or adolescents, due to the complexity and prolongation of the accompaniment required.
In view of this reality, we propose the construction of a risk card that considers variables such as the age of the caregiver, the family structure and the characteristics of the person to be cared for. This tool would make it possible to prevent situations of physical and/or emotional overload, facilitating the implementation of psychosocial support devices in various institutions. Such measures should incorporate a gender and inclusion perspective that recognizes and values the care work performed by all people, regardless of their identity or family role.
Among the limitations of this research are several considerations. First, difficulties were encountered due to the large volume of data collected, which represented a significant limitation. The exhaustive review, correction and elimination of erroneous data demanded a considerable amount of time and effort, delaying the analysis process and affecting the time available for more detailed and accurate work on the variables. This delay, in turn, interfered with the deadlines established by the doctoral program, limiting the possibility of a deeper exploration of some key aspects of the research. Second, the lack of additional variables was identified as a relevant limitation, as the absence of factors such as family dynamics, perceived support, caregiver mental health, coping techniques or caregiver motivation prevented a more comprehensive understanding of caregiver overload. These elements could explain to a greater extent the percentage of overload experienced, so it is suggested that future studies include them to provide a more complete picture of the factors involved and thus develop more effective strategies for their support. Finally, the use of a non-probabilistic sample selected by convenience represents an important limitation, since it may affect the external validity of the results and their generalizability to other populations.
At the intervention level, the risk of physical and/or emotional overload of unpaid primary caregivers could be prevented by implementing psychosocial devices in the various institutions, both public and private. The construction of a risk card that identifies the presence of variables that increase caregiver overload could be a useful tool for teams that are intervening in families that are in a vital stage associated with caregiving or that, for non-regulatory reasons, have a family member who requires care.
Acknowledgments We thank the professionals, users and participating families of the Corporación de Rehabilitación Club de Leones Cruz del Sur for their contribution to this study.
Conflict of interest: none.
References
Andela, M., Truchot, D., & Huguenotte, V. (2021). Work environment and elderly abuse in nursing homes: The Mediating Role of Burnout. Journal of Interpersonal Violence, 36, 5709-5729. https://doi.org/10.1177/0886260518803606
Arriagada, I. (2020). El trabajo de cuidados y las cuidadoras en América Latina: entre la invisibilidad y el reconocimiento. CEPAL. https://www.cepal.org/es/publicaciones/45797
Arriagada, I. (2010). La organización social de los cuidados y vulneración de derechos en Chile. ONU Mujeres-Centro de Estudios de la Mujer. http://www.cem.cl/pdf/cuidadoschile.pdf
Bauer, J. M., & Sousa-Poza, A. (2015). Impacts of informal caregiving on caregiver employment, Health, and Family. Journal of Population Ageing, 8, 113-145. https://doi.org/10.1007/s12062-015-9116-0
Bond Disability and Development Group. (2024). An intersectional approach to disability inclusion: A resource for members of the Bond Disability and Development Group, donors, and wider NGO sector. https://www.bond.org.uk/wp-content/uploads/2024/03/Bond-DDG-Intersectionality-Paper-Final-002.pdf
Breinbauer, H., Vázquez, H., & Mayanz, S. (2009). Validación en Chile de la Escala de Sobrecarga del Cuidador de Zarit de sus versiones original y abreviada. Revista Médica de Chile, 137, 657-665. http://dx.doi.org/10.4067/S0034-98872009000500009
Brummett, B. H., Babyak, M. A., Siegler, I. C., Vitaliano, P., Ballard, E. L., Gwyther, L. P., & Williams, R. B. (2006). Associations among perceptions of social support, negative affect, and quality of sleep-in caregivers and non-caregivers. Health Psychology, 25, 220-225. https://doi.org/10.1037/0278-6133.25.2.220
Comisión Económica para América Latina y el Caribe, ONU Mujeres. (2022). Hacia la construcción de sistemas integrales de cuidados en América Latina y el Caribe: elementos para su implementación. https://hdl.handle.net/11362/47898
Domínguez, J. A., Ruíz, M., Gómez, I., Gallego, E., Valero, J., & Izquierdo, M. T. (2012). Ansiedad y depresión en cuidadores de pacientes dependientes. SEMERGEN-Medicina de Familia, 38(1), 16-23. https://doi.org/10.1016/j.semerg.2011.05.013
Dong, X. (2015). Elder abuse: Systematic review and implications for practice. Journal of the American Geriatrics Society, 63(6), 1214–1238. https://doi.org/10.1111/jgs.13454
Durán, M. A., & Rogero-García, J. (2009). Los costes invisibles de la enfermedad: impacto económico de los cuidados informales en las familias. Fundación La Caixa.
Escandell-Rico, F. M., & Pérez-Fernández, L. (2022). Impacto en la salud y sus determinantes de las personas mayores cuidadoras. Atención Primaria, 54(10). https://doi.org/10.1016/j.aprim.2022.102464
Espinoza Miranda, K., & Jofre Aravena, V. (2012). Sobrecarga, apoyo social y autocuidado en cuidadores informales. Ciencia y enfermería, 18(2), 23-30. http://dx.doi.org/10.4067/S0717-95532012000200003
Flores, N., Jenaro, C., Moro, L., & Tomşa, R. (2015). Salud y calidad de vida de cuidadores familiares y profesionales de personas mayores dependientes: estudio comparativo. European Journal of Investigation in Health, Psychology and Education, 4(2), 79-88. https://doi.org/10.1989/ejihpe.v4i2.55
Folbre, N. (2021). Who cares? A feminist critique of the care economy. Rosa-Luxemburg-Stiftung. https://www.rosalux.de/fileadmin/rls_uploads/pdfs/sonst_publikationen/folbre_whocares.pdf
García, G.E. & Navarro, A. N. (2016) Psicología social y género: las familias, escuela y el trabajo como ámbitos de aplicación (pp. 171- 201). En Domínguez, J. O. N., Bernal, S. A., & García, J. M. psicologías sociales aplicadas. Editorial: Biblioteca Nueva
Gérain, P., & Zech, E. (2021). Do informal caregivers experience more burnout? A meta-analytic study. Psychology, Health & Medicine, 26, 145–161. https://doi.org/10.1080/13548506.2020.1803372
Ilse, I. B., Feys, H., de Wit, L., Putman, K., & de Weerdt, W. (2008). Stroke caregivers' strain: prevalence and determinants in the first six months after stroke. Disability and Rehabilitation, 30(7), 523-530. https://doi.org/10.1080/09638280701355645
Instituto Nacional de Estadísticas. (2018). Estimaciones y proyecciones de la población de Chile 1992-2050. https://www.ine.gob.cl/docs/default-source/proyecciones-de-poblacion/publicaciones-y-anuarios/base-2017/ine_estimaciones-y-proyecciones-de-poblaci%C3%B3n-1992-2050_base-2017_s%C3%ADntesis.pdf?sfvrsn=c623983e_6
Instituto Nacional de Estadísticas. (2025). Tablas de mortalidad de Chile 1992‑2050 (proyección de esperanza de vida al nacer: 81,4 años en 2024). Censo 2024. Santiago, Chile.
Johannesen, M., & LoGiudice, D. (2013). Elder abuse: a systematic review of risk factors in community-dwelling elders. Age and Ageing, 42, 292-298. https://doi.org/10.1093/ageing/afs195
Kahriman, F., & Zaybak, A. (2015). Caregiver burden and perceived social support among caregivers of patients with cancer. Asian Pacific Journal of Cancer Prevention, 16, 3313-3317. https://doi.org/10.7314/APJCP.2015.16.8.3313
Lamas, M. (1996). El género, la construcción social de la diferencia sexual. México, Porrúa/UNAM
Lavoz, E. E., Villarroel, V. M., Jaque, R. L., & Caamaño, P. R. (2009). Factores asociados al nivel de sobrecarga de los cuidadores informales de adultos mayores dependientes, en control en el consultorio" José Durán Trujillo", San Carlos, Chile. Theoria, 18(1), 69-79.
Ministerio de Desarrollo Social y Familia. (2023a). Resultados Encuesta de Discapacidad y Dependencia 2022 Población Adulta. Observatorio Social. https://observatorio.ministeriodesarrollosocial.gob.cl/storage/docs/endide/230128_Resultados_ENDIDE_2022(Poblacion-adulta).pdf
Lillo-Crespo, M., Riquelme, J., & Sánchez, M. (2018). Impact of informal caregiving on health and lifestyle: Analysis of caregivers of dependent elderly relatives. Clinical Nursing Studies, 6(2), 1–9. https://doi.org/10.5430/cns.v6n2p1
Ministerio de Desarrollo Social y Familia. (2023b). Resultados encuesta de discapacidad y dependencia 2022 niños, niñas y adolescentes. Observatorio Social. https://observatorio.ministeriodesarrollosocial.gob.cl/storage/docs/endide/Presentacion_Resultados_ENDIDE_2022_Poblacion_NNA_version_mayo_2023.pdf
Ministerio de Desarrollo Social y Familia. (2023c). Resultados encuesta de discapacidad y dependencia 2022 personas dependientes y necesidades de cuidado. Observatorio Social. https://observatorio.ministeriodesarrollosocial.gob.cl/storage/docs/endide/20230530_Resultados_Personas_Dependientes_Necesidades_Cuidado.pdf
Montoya, D. I. G., Machado, S. Z., & Gómez, V. U. (2018). Sobrecarga en los cuidadores principales de pacientes con dependencia permanente en el ámbito ambulatorio. Medicina UPB, 37(2), 89-96. https://doi.org/10.18566/medupb.v37n2.a02
Ovejero, A. (2013). Psicología social: algunas claves para entender la conducta humana. Madrid: Biblioteca Nueva.
Petrie-Flom Center. (2021). The feminist political economy of health justice. https://petrieflom.law.harvard.edu/2021/09/29/feminist-political-economy-health-justice/
Pinquart, M., & Sörensen, S. (2003). Differences between caregivers and noncaregivers in psychological health and physical health: A meta-analysis. Psychology and Aging, 18(2), 250–267. https://doi.org/10.1037/0882-7974.18.2.250
Sánchez M. M., & González A. J. G. (2012). Introducción al estudio de los grupos. Concepto y tipos de grupos. En M. Marín-Sánchez & R. Martinez-Pecino (Eds.), Introducción a la Psicología Social (p. 175 – 92). Pirámide. https://clea.edu.mx/biblioteca/files/original/90e031740552bba852e3efaa2143fd2a.pdf
Schulz, R., & Eden, J. (Eds.). (2016). Families caring for an aging America. National Academies Press. https://doi.org/10.17226/23606
Scott, J. (2000). El género: una categoría útil para el análisis histórico. En Lamas, M. (coord.), El género. La construcción cultural de la diferencia sexual. México UNAM.
Silva, A. R. F., Fhon, J. R. S., Rodrigues, R. A. P., & Leite, M. T. P. (2021). Caregiver overload and factors associated with care provided to patients under palliative care. Investigación y Educación en Enfermería, 39(1), e10. https://doi.org/10.17533/udea.iee.v39n1e10
Vitaliano, P. P., Zhang, J., & Scanlan, J. M. (2003). Is caregiving hazardous to one’s physical health? A meta-analysis. Psychological Bulletin, 129(6), 946–972. https://doi.org/10.1037/0033-2909.129.6.946
West, C., Lazar. M. & Kramarae, Ch. (2001). El género en el discurso, en T. Van Dijk (comp.), El discurso como interacción social, vol. 2 Barcelona, Gedisa.
Yelincic, A., & Cárcamo, R. A. (2021). Cuidadores principales informales no remunerados: ¿quiénes cuidan a niños, adultos y adultos mayores en situación de discapacidad? Rehabilitación, 55(3), https://doi.org/10.1016/j.rh.2021.03.001
Zepeda-Álvarez, P. J., & Muñoz-Mendoza, C. L. (2019). Sobrecarga en cuidadores principales de adultos mayores con dependencia severa en atención primaria de salud. Gerokomos, 30(1), 2-5.
Zarit, S. H., Reever, K. E., & Bach-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feelings of burden. The Gerontologist, 20(6), 649–655. https://doi.org/10.1093/geront/20.6.649