MLS – PSYCHOLOGY RESEARCH (MLSPR)http://mlsjournals.com/ISSN: 2605-5295 |

|
(2025) MLS-Psychology Research, 8(1), 75-89. doi.org/10.33000/mlspr.v8i1.4086
Normative data for the Pittsburgh Sleep Quality Index Scale (PSQI) in a honduran university population
Rafael Menjivar Alas
Universidad Nacional Autónoma de Honduras (Honduras)
rmenjivar05@gmail.com · https://orcid.org/0009-0003-4949-1197
Abstract: Previous studies have demonstrated the existence of pathologies that affect sleep quality in the university population. For this reason, sleep problems have been studied in Honduras using the Pittsburgh Sleep Quality Index Scale (PSQI) in its Spanish version, but there are no normative data that can be used in settings. clinical. The main objective of this study was the creation of normative data using percentiles and Z scores for the interpretation of the PSQI scale. A cross-sectional correlated study was carried out in the period from February to March 2024, using stratified probabilistic sampling, with a total of 1050 participants, institutionalized in public university centers in the northern region of Honduras. The main descriptive statistics and psychometric properties of the scale were analyzed; McDonald's omega Ω = 0.88 and Cronbach's alpha α = 0.83, and several models were tested using confirmatory factor analysis (CFA), the hierarchical model was the one that presented the best fit indices with a CFI = .962; NFI = .967; TLI = .954; SRMR = .054; RMSEA = .051, and finally normative data adjusted to the sociodemographic and clinical characteristics of the sample were generated. The PSQI scale presented adequate psychometric properties, and the normative data generated could be used in decisions making regarding the sleep health of college students.
Keywords: Sleep quality, normative data, PSQI scale, psychometric properties, honduran university students.
Datos normativos para la Escala Pittsburgh Sleep Quality Index (PSQI) en población universitaria hondureña
Resumen: En estudios previos se ha demostrado la existencia de patologías que afectan la calidad del sueño en población universitaria. Por esta razón, en Honduras se han estudiado los problemas del sueño mediante la utilización de la escala Pittsburgh Sleep Quality Index (PSQI, por sus siglas en inglés) en su versión castellana, pero no existen datos normativos que puedan usarse en entornos clínicos. El objetivo principal de este estudio fue la creación de datos normativos mediante percentiles y puntuaciones Z para la interpretación de la escala PSQI. Se realizó un estudio correlacionado de corte transversal en el periodo de febrero a marzo del año 2024, utilizando un muestreo probabilístico estratificado, con un total de 1050 participantes, institucionalizados en centros universitarios públicos de la región norte de Honduras. Se analizaron los principales estadísticos descriptivos y las propiedades psicométricas de la escala; omega de McDonald Ω = 0.88 y un alpha de Cronbach α = 0.83, y se probaron varios modelos mediante el análisis factorial confirmatorio (AFC), el modelo jerárquico fue el que presentó mejores índices de ajuste con un CFI = .962; NFI = .967; TLI = .954; SRMR = .054; RMSEA = .051, y por último se generaron datos normativos ajustados a las características sociodemográficas y clínicas de la muestra. La escala PSQI presentó propiedades psicométricas adecuadas, y los datos normativos generados podrían ser utilizados en la toma de decisiones con respecto a la salud del sueño de los estudiantes.
Palabras clave: Calidad del sueño, datos normativos, escala PSQI, propiedades psicométrica, estudiantes universitarios hondureños.
Introduction
The quality of sleep has been defined by several authors as the act of sleeping well, especially during the night period in order to after a good rest, have an optimal functioning in the daytime period, and being an indispensable function for life is an important component that determines good health, this fact is conducive to an optimal quality of life (Becerra et al., 2018; Corredor Gamba and Polanía Robayo, 2020; Gellis and Lichstein, 2009; Murawski et al., 2018).
Escobar & Liendo, 2012; Resnick et al., 2003; Sato-Shimokawara et al., 2016; Virend and Somers, 2005 as cited in Becerra (2018) indicate to us that having an adequate quality of sleep will be significantly reflected in an improvement of the quality of life, since this reduces the probability of suffering certain problems such as cardiovascular, neuroendocrine, as well as cognitive and emotional.
On the other hand, sleep has been recognized as an essential factor of great importance in the lives of human beings, since it directly influences physiological and intellectual development and interpersonal relationships, through which people reach a full balance (Becerra et al., 2018; Rebok and Daray, 2024). Likewise, for Echeverry and Escobar, 2009 as cited in Becerra et al., (2018) the study of sleep is complex and is still in its infancy, but despite this, it has been determined that sleep and its quality are related to various factors such as age, sex, lifestyle, as well as the state of physical and mental health.
It should be taken into account that some changes in sleep physiology are accompanied by individual characteristics, such as bedtime and length of sleep. A person is said to be in good sleep health when there is adequate duration, efficiency is sufficient, and the level of satisfaction with sleep makes the person feel capable and fully functional throughout their day (Murawski et al., 2018). In line with the above, it can be said that the quality of sleep is not simply limited to circumstances, or physical characteristics of the person, since, it is also related to their daily life, development and performance (Becerra et al., 2018; Escobar Córdoba and Eslava-Schmalbach J., 2005).
College students are exposed to suffer more frequently from sleep problems (Hershner S.D. and Chervin R.D., 2014 as cited in Suardiaz-Muro et al., 2020). In this population some specific factors are added, on the one hand, the academic demands inherent to university studies, which involve more dedication and effort than in previous stages, and, on the other hand, non-academic ones such as working to support oneself, which involve added effort, and added to this the use of psychotropic substances and the abuse of modern technologies are also factors to be taken into account in the onset of such sleep problems (Suardiaz-Muro et al., 2020).
Because sleep influences areas such as learning, memorization capacity, some physiological processes, and the restoration of collected information, it is important to achieve and maintain a good quality of sleep in college students. However, most of them must meet academic demands that force them to extend their waking period frequently, which has an impact on their sleep-wake cycle, thus reducing the rest time they require every night (Sabillón Maldonado, L. N. et al., 2020).
The Pittsburgh Sleep Quality Index (PSQI) was used for this study, since this instrument is used to diagnose sleep quality and sleep disorders in clinical populations as well as in other research protocols in diverse populations. With young adults it has been used in some studies such as in the creation of the scale by Buysse and his collaborators, and in the adaptation of the scale in its Spanish version, among others (Royuela Rico and Macías Fernández, 1997). This scale has also been adapted in a Latin American context, specifically in Colombia (Escobar Córdoba, 2005).
The PSQI instrument consists of self-report derived questions, which in turn form seven clinically derived components of sleep difficulties; subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction. In this study, the psychometric properties were analyzed for the sample and it was determined that they are adequate and also similar to those obtained in the creation of the scale, in the adaptation to Spanish and in the adaptation in Colombia (Buysse et al., 1989; Escobar, 2005; Royuela Rico and Macías Fernández, 1997).
This questionnaire has been widely used in various regions of the world and in diverse populations. In Paraguay, a study was conducted using the ICSP questionnaire to determine the quality of sleep of medical students at the Universidad del Pacifico. A total of 158 students participated in the study, 77.08% of whom were female (n=123). This study identified a frequency of poor sleepers of 56.96%, 21.53% used hypnotic drugs to sleep (34/158). The study concludes that in this sample the number of poor sleepers is very high, proposing some strategies to improve the quality of their sleep (Núñez Bael et al., 2024).
In Mexico, a study was conducted to determine the factorial structure and internal consistency of the ICSP in university athletes in order to evaluate the psychometric properties of the instrument. The study was a non-experimental cross-sectional study with 98 college athletes aged 17-25 years. The internal consistency and homogeneity of the instrument were analyzed, as well as the AFE and the AFC. Reliability showed a Cronbach's alpha of 0.79, and the AFC provided an adapted unidimensional model, eliminating the medication use and habitual sleep efficiency components (Favela-Ramirez et al., 2022).
Sabillón Maldonado et al., (2020) conducted a study in a Honduran population with 317 students with the aim of generating evidence on sleep quality and excessive daytime sleepiness in medical and surgical students, in the third academic term of 2019. We worked with two instruments applied simultaneously, the Pittsburgh Sleep Quality Index (PSQI) and the Epworth Sleepiness Scale. We worked with 195 women (61.5%) and 122 men (38.5%), whose mean age was 19.5 years for both. The average ICSP was 9.61, within the range of poor sleep quality that warrants medical attention and treatment.
There were no significant differences in the ratings by gender. A bilateral significance level for the ICSP of p = 0.405 was generated, accepting the null hypothesis, since there were no significant differences in the scores of both sexes. Finally, an important conclusion is that it was demonstrated that there are indeed problems with respect to sleep quality in medical and surgical students, which could have repercussions on their work as licensed professionals in the future (Sabillón Maldonado et al., 2020).
Bustamante-Ara et al. (2020) conducted a study in a Chilean population with 278 university students, with the aim of evaluating the association between academic performance, physical activity and sleep quality, and also to determine the existing differences according to gender in Physical Education Pedagogy students during the covid-19 pandemic. The sleep quality of the undergraduates scored 8.4 ± 3.3 points, which was 3 points above the criteria for good baseline sleep quality. In this aspect, women reported a higher score compared to men (p = 0.004).
In the US population in the state of California, a study was conducted to evaluate the factor structure of the Pittsburgh Sleep Quality Index (PSQI). The sample included 107 elderly patients with rheumatoid arthritis. The AFC evaluated one-, two- and three-factor models. The unidimensional model yielded a poor fit to the data obtained from the sample. On the other hand, the three-factor model obtained the best fit indices, being the two-factor model; sleep efficiency and perceived sleep quality, the one that presented the best psychometric properties since its fit indices were very good, and likewise the individual reliability was acceptable (Perry et al., 2014).
Lezcano H. et al., (2014) conducted a study in Panama Determining the characteristics and quality of sleep in medical students at the University of Panama. This study was descriptive, cross-sectional, and consisted of 290 students. Data collection was performed using the Pittsburgh Sleep Quality Index (PSQI). A total of 56.6% (164) were female. This study concluded that most of the subjects included in the sample are poor sleepers.
In 2005 Escobar-Córdoba and Eslava-Schmalbach carried out the Colombian validation of the Pittsburgh Sleep Quality Index (PSQI), taken from the original article and the Spanish version. To this end, the instrument was reviewed by experts and subsequently two pilot studies were carried out with 104 subjects in the city of Bogotá between 6 and 90 years of age. It is important to note that modifications were made to questions 5, 8, 9 and 10 of the Spanish version, although it is already an adaptation in a common language, it presented terms that did not have the same interpretation in local conditions.
In accordance with studies previously conducted in the Latin American region with university students and specifically with the study conducted by Sabillón Maldonado et al. (2020) in a university in the northern part of Honduras using the PSQI, in which medical students between 18 and 25 years of age of both sexes participated, it was decided to conduct a study with this age group with the purpose of studying this problem in greater depth. For all these reasons, the present study was carried out with a sample of institutionalized students in university centers, with the main objective of creating normative data according to the influential variables identified with the multiple linear regression technique.
Method
Research Design
This study according to its approach is quantitative, because it presents a set of processes, and at the same time involves the collection of data in order to test previously established hypotheses based on numerical measurement and statistical analysis, with the aim of testing theories (Hernández Sampieri et al., 2014). According to its depth it is of a correlational type, since it measures the degree of relationship or degree of association that exists between the sleep quality of the subjects included in the sample and the sociodemographic variables (Hernández Sampieri et al., 2014).
According to its temporality, it is of cross-sectional type, because the data collection was performed by applying the Pittsburgh Sleep Quality Index (PSQI) scale at a single time to estimate the quality of sleep, or sleep problems affecting the target population in the last month, likewise the prevalence of sleep disorders of the participants included in the sample was determined. (Hernández Sampieri et al., 2014).
According to the type of source, this is a field study, because it was carried out by applying a questionnaire directly to the participants from whom the information was obtained. For its purpose it is applied, since its ultimate aim was to determine the existence of sleep quality from the application of the Pittsburgh Sleep Quality Index (PSQI) instrument, in order to establish criteria to assess this variable (Hernández Sampieri et al., 2014).
Participants
The sample consisted of 1050 participants, where 35.33% identified themselves as men and 64.67% as women, with an age range between 17 and 60 years (M = 24.76; SD = 8.66). The subjects included in the sample are students institutionalized in centers of the National Autonomous University of Honduras (UNAH), northern zone. Of the participants, 22.67% were married, and 77.33% were unmarried. A total of 8.67% were pursuing graduate studies, and 91.33% were pursuing undergraduate studies. 5.05% were enrolled in UNAH/Tela, 5.33% in UNAH/La Ceiba, 8.67% in UNAH/El Progreso, and 80.95% in UNAH/Cortés. Stratified probability sampling was used for this study.
Instrument
The Pittsburgh Sleep Quality Index (PSQI) originally developed by Buysse et al. (1989) is a Likert-type scale that assesses qualitative and quantitative aspects of sleep quality in the month prior to its application. In the original publication, the scale was reported to have an internal consistency (Cronbach's alpha) of 0.83. Cut-off point 5 correctly identified 88.5% (131/148) of all patients and controls (kappa = 0.75), (p = 0.001), with a sensitivity of 89.6%, and specificity of 86.5%.
It was adapted to Spanish by Royuela Rico and Macías Fernández (1997) with the aim of establishing its clinimetric properties and validating it in the Spanish population. Good psychometric results were obtained both in the sample that included young people and in the segment of older adults, which makes this instrument suitable for epidemiological and clinical research on sleep disorders. The Spanish version of the PSQI instrument had a Cronbach's alpha internal consistency of 0.81; the Kappa coefficient was 0.61; the sensitivity was 88.6%; the specificity was 74.9%; and the predictive value of the positive test was 80.7 (p. 81).
This questionnaire was adapted in Colombia by Escobar Córdoba, (2005) taking the original questionnaire (PSQI) and the Spanish validation of the Pittsburgh Sleep Quality Index (PSQI). A first expert consensus was then reached with five renowned physicians specialized in sleep disorders to create the Colombian version of the ICSP-VC. Subsequently, it was applied as a pilot test for the respective linguistic and cultural validation. The criterion and concurrent validity of the test showed that the ICSP-VC is able to find differences in its scores between subjects with clinical characteristics of poor sleepers, hypnotic users and older adults (Escobar Cordoba, 2005).
The ICSP-VC is a short, simple and well-accepted questionnaire that identifies 'good' and 'bad' sleepers, does not provide a diagnosis and serves for screening the subjects included in the sample. In psychiatric patients it can identify concomitant sleep disorders. It is also important to bear in mind that the results obtained guide the physician to the most disturbed aspects of sleep and the need to seek help. In addition, it serves to monitor the clinical course of sleep disorders, the influence on the course of mental entities and the response to treatment (Escobar Córdoba, 2005).
The instrument is composed of 24 questions, 19 of which are answered by the subject and 5 by the roommate. The first 4 (bedtime, or how long the subject thinks he/she actually sleeps during the night) should be answered concretely. The remaining 20, including those to be answered by the roommate, which ask about aspects such as the quality of sleep the subject claims to have, or the frequency of certain events (difficulties in falling asleep or the presence of nightmares) are answered using an ordinal scale with four grades. The time to answer it is 5 to 10 minutes (Royuela Rico and Macías Fernández, 1997).
The scale is composed of seven components; subjective sleep quality (the number of hours a person considers that he/she has slept), sleep latency (the period in minutes, which elapses from the moment the individual goes to bed and the onset of sleep), sleep duration (actual hours slept), habitual sleep efficiency (the percentage between the actual number of hours slept and the number of hours a person stays in bed), sleep disturbances (difficulty in sleeping), sleep disturbances (difficulty in falling asleep), the use of hypnotic drugs, and daytime dysfunction (Royuela Rico and Macías Fernández, 1997).
According to Royuela Rico and Macías Fernández, (1997) to correct this questionnaire, only the first 18 questions that correspond to the items answered by the subject under study are evaluated. The question that asks whether the subject sleeps alone or in company, and those asked to the bed or roommate are not scored, and only serve as information on aspects such as the frequency of snoring, apneas, convulsions, or confusional episodes. The correction of each questionnaire takes approximately five minutes.
Seven scores are obtained from the corrections, each of these components receiving a discrete score ranging from 0 to 3. A score of 0 indicates no sleep problems, while a score of 3 indicates serious problems. The sum of the scores obtained in each of the partial components generates a total score (PT), which can range from 0 to 21. According to Buysse, et al., a total score (PT) equal to 5 is the cut-off point, therefore a score equal to or below 5 is the indicator of good sleepers and above 5 bad sleepers. In this study we used the version adapted to Spanish (Royuela Rico and Macías Fernández, 1997).
Procedure
The study conformed to the ethical guidelines of the Helsinki declaration of the world medical association (World Medical Association, 2013, Standard 25). Before beginning the interview and to ensure the anonymity, confidentiality, consent and voluntariness of the participants, they were provided with an informed consent form, which they had to sign as a sign of conformity. If participants were unable to give their consent, they were excluded from participating in the study.
Data were collected by applying the Pittsburgh Sleep Quality Index (PSQI) scale in February and March 2024. The instrument was applied in self-report format, both in person and online. The time for the application of the questionnaire was between 5 to 10 minutes.
For the study of the data, a frequency analysis was performed and the main descriptive statistics were applied. In addition, reliability analyses were performed for internal consistency (Cronbach's alpha and McDonald's omega) to determine the good performance of the items and validity analyses to determine the factorial structure of the test by means of confirmatory factor analysis (CFA), and finally, normative data were created in order to characterize the sample and describe the variables studied.
Data Analysis
The Rstudio program was used to perform all statistical calculations, and the Statistical Package for Social Sciences (SPSS) was used to compare the results. A calculator was also created to obtain the exact percentile using the total score of the PSQI scale, which was performed in Microsoft Excel.
Confirmatory factor analysis (CFA) calculation was performed, to obtain the model specification, identification (factor structure), parameter estimation, model fits (NFI, TLI, CFI, RMSR, RMSEA), and finally interpretations of each model were performed (Bahri Yusoff, 2019). The fit indices were calculated using the Weighted Least Square Mean and Variance estimator (WLSMV). Reliability was tested for internal consistency, using Cronbach's alpha coefficient, and McDonald's omega for each factor and the PSQI total score (Bahri Yusoff, 2019; Sattler, 2010).
To determine the normative data, the best explanatory model for the data was identified. Age and sex were included as predictor variables for the final model, considering a value of p ≤ 0.05 as acceptable. The mixed (both) elimination system was used to incorporate the variables in the model.
For the establishment of the normative data for the Pittsburgh Sleep Quality Index (PSQI) scale, the regression analyses performed tested the assumptions of: Multicollinearity; VIF < 10, presence of influential values; by Cook's distance test, considering a value < 1 acceptable. Homoscedasticity; using the Breusch-Pagan test and a value of p ≥ 0.05 was considered acceptable. Normality; using the Lilliefors test (based on Kolmogorov-Smirnov), taking a value of p ≥ 0.05 as acceptable.
The normative data for the PSQI were established using the linear regression methodology and the standard deviation of the residual values of the model, proposed by Van Breukelen and Vlaeyen, (2005); Van der Elst et al., (2012) this allows generating normative data adjusted to sociodemographic and clinical variables, in four steps:
1. The predictive value (Ŷ𝑖) of the score was calculated from the beta parameters (B), i.e. the predictors established in the final model with the formula: Ŷ𝑖 = B0 + B1X1+ B2X2 +...BkXk.
2. The residual value is calculated by subtracting the predictive value (Ŷ𝑖) from the direct PSQI score, according to the following formula: 𝑒𝑖 = Y𝑖 - Ŷ𝑖.
3. The residual value obtained (zi) is standardized by dividing the residual value (𝑒𝑖) by the residual standard deviation (DT𝑒), z𝑖= 𝑒𝑖/DT𝑒.
4. Using the standard normal cumulative distribution, we proceeded to calculate the exact percentile value corresponding to the previously calculated (Z) value, or through the empirical cumulative function of the standardized residuals.
Results
Descriptive statistics were calculated for the seven components and total score of the Pittsburgh Sleep Quality Index (PSQI) scale. It was found that the mean of the components obtained values of 0.43 and 1.23, the component with the highest score was, sleep latency (1.23 ± 0.96), and the lowest was the use of hypnotics (0.43 ± 0.93). The range obtained a value of 3 for the first six components and their asymmetries were positive, while for the daytime dysfunction component the range was 2 and the asymmetry was negative. The total PSQI presented a mean of (7.44 ± 3.37), a range of 17, and a positive skewness. The kurtosis was positive for three of the factors and negative for four of them and the total score.
Structural Validity
The CFA was performed to test models tested in other studies. The unidimensional model, unidimensional model adapted by eliminating component 6 (use of hypnotics), correlated model with two main factors and the hierarchical model were tested. The hierarchical model was the best fit for the PSQI scale in the sample studied with Honduran university students; all components had standardized coefficients and significants. In the hierarchical model, a main factor called the Pittsburgh Sleep Quality Index (PSQI) was proposed, with 3 second-order factors: sleep efficiency (SE), PSQ = perceived sleep quality; SDP = daily sleep disturbances.
The 7 components were included in this model: sleep duration (SD), habitual sleep efficiency (EHS), hypnotic use (UH), subjective sleep quality (SSQ), sleep latency (SL), sleep disturbances (SD), and daytime sleep dysfunction (DSD). The model fit indices were calculated using the Weighted Least Square Mean and Variance (WLSMV) estimator, showing adequate values (see Figure 1).
Figure 1
Hierarchical scale model (PSQI) with college students.
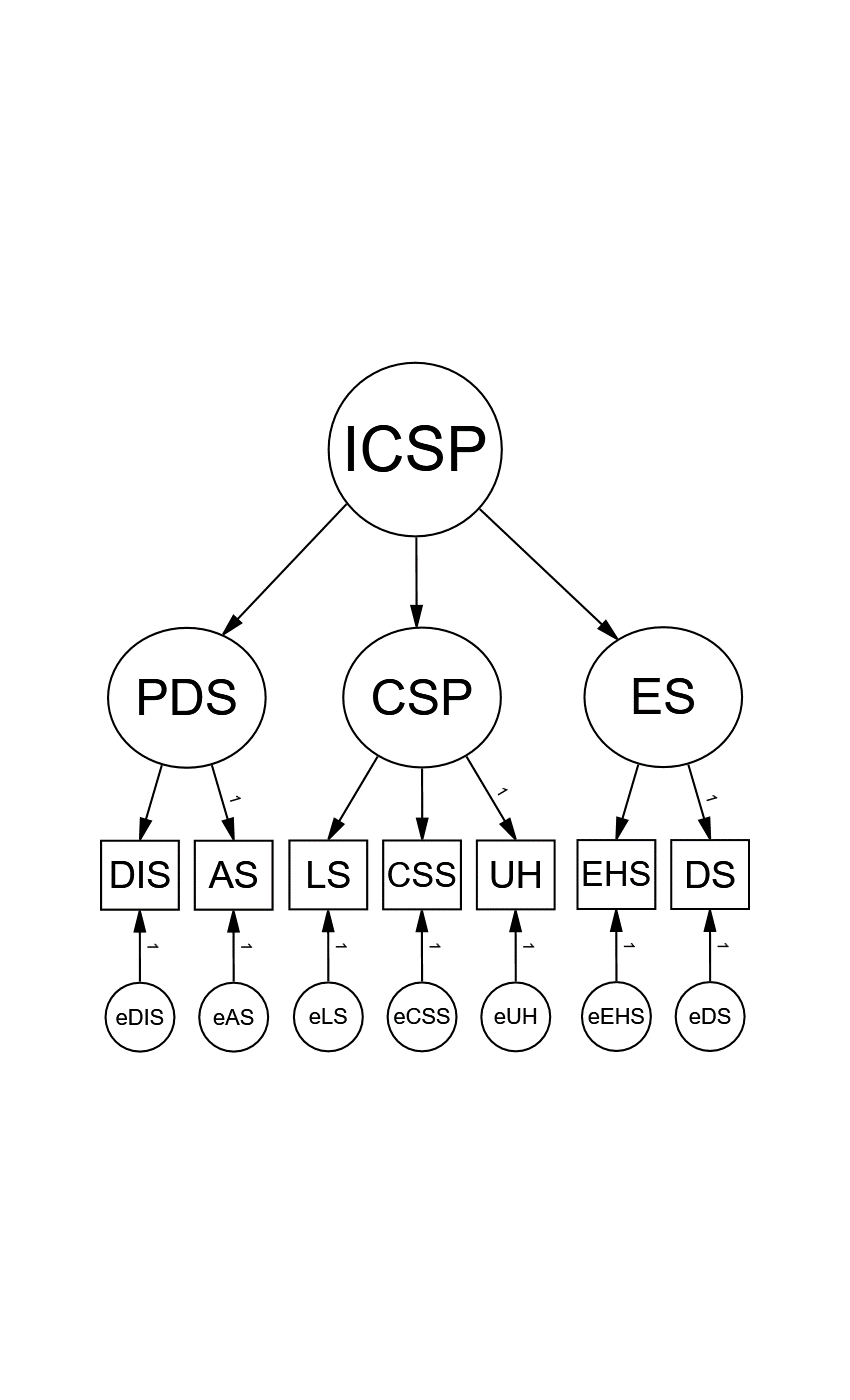
Note. All standardized coefficients and error values significant, p < .05, and adequate factor loadings ≥ 0.36 for all scale components.
Table 1
Fit indices of the models tested.
| Adjustment Ratios |
Models |
|||
|
A factor |
An adapted factor |
Correlated |
Hierarchical |
|
| X2 (df) |
128.684 (14) |
110.675 (9) |
88.009 (12) |
87.120 (11) |
| P |
.000 |
.000 |
.000 |
.000 |
| IFC |
.943 |
.932 |
.962 |
.962 |
| NFI |
.937 |
.927 |
.957 |
.967 |
| TLI |
.915 |
.887 |
.934 |
.954 |
| SRMR |
.079 |
.071 |
.064 |
.054 |
| RMSEA (90% CI) |
.088 |
.104 |
.078 |
.051 |
Note. X2 = chi-square; df = degrees of freedom; CFI = comparative fit index; NFI = normed fit index; TLI = Tucker-Lewis index; SRMR = standardized root mean square residual; RMSEA = root mean square error of approximation; CI = confidence interval.
The fit indices for the models tested had to meet certain criteria to determine if they are adequate. An adequate CFI, NFI and TLI should have presented values ≥ 0.90, the RMSEA and SRMR < 0.08 (Kline, 2016; Tabachnick and Fidell, 2014 as cited in Maldonado, 2019). The one-factor model presented adequate CFI, NFI, TLI and SRMR while the RMSEA did not fit, the fitted one-factor model showed acceptable values of CFI, NFI, SRMR, but TLI and RMSEA did not fit. In the correlated model of the items with two main factors (sleep efficiency and perceived sleep quality), it revealed adequate values for almost all the fit indices, with the exception of RMSEA.
A hierarchical model of the items with three factors (sleep efficiency, perceived sleep quality and daily sleep disturbances) was also considered, which revealed adequate fit indices. Reporting adequate factor loadings for all components > .30. The habitual sleep efficiency factor showed a mean equal to M = 0.584 and SD = 0.170, the perceived sleep quality factor showed M = 0.539 and SD = 0.108), and the daily sleep disturbances factor showed M = 0.868 and SD = 0.063).
Reliability
Reliability was calculated by internal consistency using Cronbach's alpha and McDonald's omega, with the objective of verifying whether the items and each factor of the scale presented an acceptable degree of correlation with the total scores. For this purpose, internal consistency reliability was calculated by means of a polychoric matrix of the items. Cronbach's alpha coefficient for the total score was α = 0.83, and the McDonald omega total was Ω = 0.88.
Subsequently, Cronbach's alpha and McDonald's omega were calculated for each second-order factor of the hierarchical model that was previously tested with confirmatory factor analysis (CFA). The sleep efficiency factor obtained values of (Ω = 0.82 and α = 0.73). On the other hand, the daily sleep disturbances factor yielded the highest scores, a McDonald omega of Ω = 0.88, and a Cronbach's alpha of α = 0.83; while the perceived sleep quality factor showed the lowest values (Ω = 0.76 and α = 0.73).
Regulatory Data
The variables taken into account in the final model were age and sex, both variables presented a highly significant statistical significance with values (p = 0), and explained 14% of the variance of the total score of the PSQI scale (see Table 2). The multiple linear regression technique was determined as the best explanatory model.
The results showed that the variables centralized age, quadratic age, university center, education, and marital status were not predictor variables of the PSQI total score, since they did not show adequate statistical significance, obtaining p values > 0.05, so they were discarded, and the multiple linear regression analysis was performed again, applying the mixed elimination procedure (both) for the incorporation of the variables in the analysis.
For the establishment of the PSQI normative data, the regression analyses performed tested the assumptions of: Multicollinearity; VIF ≤ 1.0045, presence of influential values; by Cook's distance test p = 0.009, homoscedasticity; by Breusch-Pagan test p = 0.121. Normality; by Lilliefors test (based on Kolmogorov-Smirnov), p = 0.071. After checking for compliance with the assumptions, normative data were generated with the four-step procedure in order to provide the clinician with the ability to determine an accurate percentile for a participant who has a specific PSQI score.
The calculation of the exact percentile from the direct score of the PSQI was performed according to Van Breukelen and Vlaeyen, (2005), for which the following four steps should be followed:
Step 1. The predictive value (Ŷ𝑖) of the score is calculated from the beta parameters (ß), established in the final multivariate model (see Table 2).
Step 2. The residual value (𝑒𝑖) is calculated by computing the difference between the direct score obtained (PSQI total score) (Y𝑖) and the predictive value calculated in step 1.
Step 3. The residual value (𝑒𝑖) obtained should be standardized (Zi), using the standard deviation (SD𝑒) of the model.
Step 4. The standardized value (Zi) calculated in step 3 can be transformed to its corresponding percentile. A normative data calculator can be created for this model or a normal cumulative distribution. In this case it should be noted that the standardized residual values had a normal distribution.
Table 2
Final multivariate model for the Pittsburgh Sleep Quality Index (PSQI) score
|
Score |
Predictors |
ß |
Standard Error |
t |
p-value |
R2 Adjusted |
|
|
Total score of the ICSP |
Constant |
5.5619 |
0.3460 |
16.074 |
< 2e-16 |
*** |
0.147 |
| Age |
0.0393 |
0.0118 |
3.339 |
0.000 |
*** | ||
| Sex |
1.3993 |
0.2133 |
6.561 |
8.4e-11 |
*** | ||
Note. Predictor variables (age and sex), using the PSQI total score as the criterion variable.
Table 3 presents the normative data obtained according to gender, showing the percentile (Pc), the direct scale score (PD), and the Z scores. Women presented a larger sample (679), with a mean for this group of (7 ± 3.37), while for the men's group the sample was (371) and a mean of (6 ± 3.36).
Table 3
Normative data of the Pittsburgh Sleep Quality Index (PSQI) scale as a function of gender
| Pc | Men | Women | Pc | ||
| PS | Z | PS | Z | ||
| 99 | 13 - 21 | 2.292 | 14 - 21 | 2.170 | 99 |
| 98 | 12 | 1.988 | 13 | 1.867 | 98 |
| 95 | 11 | 1.684 | 12 | 1.563 | 95 |
| 90 | 9 - 10 | 1.077 | 11 | 1.259 | 90 |
| 80 | 8 | 0.773 | 10 | 0.956 | 80 |
| 70 | 7 | 0.470 | 8 - 9 |
0.348 |
70 |
| 50 | 6 | 0.166 | 7 |
0.045 |
50 |
| 45 | 5 | -0.138 | 6 |
-0.259 |
45 |
| 30 | 4 | -0.441 | 5 |
-0.563 |
30 |
| 20 | 3 | -0.745 | 4 |
-0.866 |
20 |
| 15 | 2 | -1.960 | 3 |
-1.170 |
15 |
| 10 | 1 | -2.263 | 1 - 2 |
-2.081 |
10 |
|
|
|
|
|
|
|
| n | 371 | 679 |
|
||
| M | 6 | 0.242 | 7 | 0.272 |
|
| DE | 3.36 | 1.448 | 3.37 | 1.321 |
|
Note. n = sample, SD = standard deviation, M = mean.
Discussion and Conclusions
According to the results obtained by applying the Pittsburgh Sleep Quality Index (PSQI) scale, it was found that university students present sleep problems. Therefore, it is considered important for people who have sleep problems to take this into consideration in order to avoid major problems in the future. The above described is supported by previous studies that have shown the association between low sleep quality with different mental health disorders such as cognitive problems, psychiatric disorders such as anxiety and depression, as well as physical and cardiovascular risk, among others (Ferré-Masó A. et al., 2020).
Women presented higher means than men in the measurement of sleep quality variables, which evidences a greater deterioration of their sleep, although when analyzed without discriminating by gender, a mean of 7.44 was found in the total score of the ICSP scale. The above described indicates that in the evaluated subjects there is a need for attention and health counseling in order to improve habits related to sleep hygiene, being consistent with what has been reported in previous studies indicating the prevalence of some sleep problems in young people with a greater extent in women (Bustamante-Ara et al., 2020; Favela-Ramírez et al., 2022; Murawski et al., 2018; Núñez Bael et al., 2024; Royuela Rico et al., 2000; Sabillón Maldonado, L. N. et al., 2020).
It was concluded that in the sample studied with university students, the older they were, the greater the deterioration in the quality of their sleep, and it was also evidenced that married students presented greater complications with sleep health in comparison with single students. As for the variable’s university center and level of schooling, there were no significant differences in the means.
After analyzing the structural validity of the Pittsburgh Sleep Quality Scale (PSQS) by confirmatory factor analysis (CFA), with the testing of four models, it was shown that the hierarchical model with 3 factors (sleep efficiency, perceived sleep quality and daily sleep disturbances), presented appropriate fit indices, as did the study conducted in Belgium with patients with chronic fatigue index (Mariman et al., 2012). For this reason, this model is suggested for the assessment of sleep quality with the PSQI scale in Honduran university students.
Reliability was calculated using McDonald's omega and Cronbach's alpha for the hierarchical model, which showed adequate values for each factor and for the total score, as in the original study proposed by Buysse et al. (1989), the adaptation of the scale to the Spanish version by Royuela Rico and Macías Fernández (1997), and the Colombian adaptation by Escobar Cordoba (2005), which leads to the conclusion that the scale presents adequate psychometric properties for the sample of university students.
The Colombian version of the Pittsburgh Sleep Quality Index (PSQI) scale (ICSP-VC) was used for this study, which proved to be a useful tool for the clinician in making decisions regarding the sleep health of Honduran university students, since it not only takes into account clinical judgment, but also the opinion of the subjects themselves. After the respective psychometric analyses carried out throughout this study, it became evident that the use of this scale in the assessment of sleep quality in university students is adequate since it collects relevant information related to the health of the subjects included in the sample.
The main objective of this study was to generate normative data for the interpretation of the Pittsburgh Sleep Quality Index (PSQI) test in the Honduran university population, specifically in the centers of the Universidad Nacional Autónoma de Honduras (UNAH) northern zone. It was found that gender variables are related to test scores, which was determined by regression analysis to generate these normative data, which could be very useful in the assessment of sleep quality in university students. The variable that presented differences in the scores was gender (male, female), where the female group presented higher means.
The normative data obtained in this study are of significant value for practical application in both clinical and educational settings. In the clinical context, these data may serve as a point of comparison for early identification of sleep disturbances in college students. Mental health and sleep professionals could use these data as a reference for the purpose of detecting deviations from patterns considered normal in the target population, facilitating the implementation of personalized interventions.
In the educational setting, these results could serve as a basis for the design and implementation of programs to promote sleep hygiene in the university population. In line with the above, workshops led by health professionals could be implemented for the university population, with the purpose of providing strategies to regulate the circadian rhythm and reduce the use of screens before going to bed. Universities could institute information campaigns within their student welfare systems aimed at raising awareness of the relationship between sleep quality and academic performance.
The normative data generated in this study should be interpreted with the following limitations in mind; because the participants were students at the National Autonomous University of Honduras (UNAH) from four centers in the northern region of Honduras, the normative data presented should not be generalizable to non-university students who do not live in the region, persons under 17 years of age and over 60 years of age, or subjects whose native language is not Spanish. This study considered a sample of 1050 subjects, from university centers in the north of the country; for future studies, it is recommended that the geographic area be expanded to a national level and a larger sample be used.
This study did not include the relationship between psychiatric and physical pathologies and poor sleep quality in the academic context of university students; therefore, it is recommended that future researchers continue to investigate further to demonstrate the association between these constructs. It is also recommended to consider the application of the Athens and Oviedo scales, using their scores, to specifically detect disorders such as insomnia that affect sleep quality to a greater extent. It would also be important to study the influence of music as a therapy to reduce stress and anxiety levels, and thus improve the quality of sleep in this population.
Acknowledgments
Special thanks are extended to the professors and administrative personnel of the National Autonomous University of Honduras (UNAH), who were involved in the application of the instrument, as well as in the processing of the respective permits for its application; these personnel are part of the staff of the university centers financed by the university centers.
References
Bahri Yusoff, M. (2019). ABC of Content Validation and Content Validity. Education in Medicine Journal, 11(2),49-54. https://doi.org/10.21315/eimj2019.11.2.6
Becerra, J., Martinetti, L., Mogollón, M., y Vargas, E. (2018). Calidad de sueño en pacientes con hemodiálisis. Revista venezolana de enfermería y ciencias de la salud, 11(2), 99-106. https://revistas.uclave.org/index.php/sac/article/view/2213
Bustamante-Ara, N., Russell, J., Godoy-Cumillaf, A., Merellano-Navarro, E., & Uribe, N. (2020). Rendimiento académico, actividad física, sueño y género en universitarios durante la pandemia 2020. Cultura, Ciencia y Deporte, 17(53), 109-131. https://doi.org/doi.org/10.12800/ccd.v17i53.1897
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, and Kupfer DJ (1989). The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Research. 28(2), 193-213. https://doi.org/10.1016/0165-1781(89)90047-4
C. Cole, J., J. Motivala, S., J. Buysse, D., N. Oxman, M., J. Levin, M., and R. Irwin, M. (2006). Validation of a 3-Factor Scoring Model for the Pittsburgh Sleep Quality Index in Older Adults. Sleep, 29(1), 112-116. https://doi.org/10.1093/sleep/29.1.112
Corredor Gamba, S., y Polanía Robayo, A. (2020). Calidad del Sueño en Estudiantes de Ciencias de la Salud, Universidad de Boyacá (Colombia). Medicina, 42(1), 8-18. https://doi.org/10.56050/01205498.1483
Daniel J. Buysse, Charles F. Reynolds, Timothy H. Monk, Carolyn C. Hoch, Amy L. Yeager, y David J. Kupfer (1991). Quantification of Subjective Sleep Quality in Healthy Elderly Men and Women Using the Pittsburgh Sleep Quality Index (PSQI), Sleep, 14(4), 331-338. https://doi.org/10.1093/sleep/14.4.331
Escobar Córdoba, F. (2005). Validación colombiana del índice de calidad de sueño de Pittsburgh. Revista Neurológica, 40(3), 150-155. DOI:10.33588/rn.4003.2004320
Favela-Ramírez, C, Castro-Robles, AI, Bojórquez-Díaz, CI, y Chan-Barocio, NL. (2022). Propiedades psicométricas del índice de calidad del sueño de Pittsburgh en deportistas. RICCAFD, 11(3), 29-46. https://doi.org/10.24310/riccafd.2022.v11i3.15290
Ferre-Masó A., Rodríguez-Ulecia Inmaculada, y García-Gurtubay Iñaki. (2020). Diagnóstico diferencial del insomnio con otros trastornos primarios del sueño comórbidos. Atención Primaria, 52(5),345-354. https://doi.org/10.1016/j.aprim.2019.11.011
Genchi, A. J. (2013). Características clínicas y diagnósticos de insomnio de acuerdo con la Clasificación Internacional de Trastornos del Sueño en la práctica médica mexicana. Revista Mexicana de Neurociencia, 14(4), 183-190. https://www.medigraphic.com/pdfs/revmexneu/rmn-2013/rmn134c.pdf
Hernández Sampieri, R., Fernández Collado, C., & Baptista Lucio, M. (2014). Metodología de la investigación. Mexico D.F,McGRAW-HILL / Interamericana Editores S.A. DE C.V.
Jiménez Genchi, A., Monteverde-Maldonado, E., Nanclares-Portocarrero, A., Esquivel-Adame, G., y De la Vega-Pacheco, A. (2008). Confiabilidad y análisis factorial de la versión en español del índice de calidad de sueño de Pittsburgh en pacientes psiquiátricos. Academia Nacional de Medicina de México, 144(6), 491-496. https://www.medigraphic.com/pdfs/gaceta/gm-2008/gm086e.pdf
Lezcano, H., Vieto, Y., Morán, J., Donadío, F., y Carbonó, A. (2014). Características del Sueño y su Calidad en Estudiantes de Medicina de la Universidad de Panamá. Revista médico científica, 27(1), 3-11. https://revistamedicocientifica.org/index.php/rmc/article/view/386
Mariman, A., Vogelaers, D., Hanoulle, I., Delesie, L., Tobback, E., y Pevernagie, D. (2012). Validation of the three-factor model of the PSQI in a large sample of chronic fatigue syndrome (CFS) patients. Journal of Psychosomatic Research, 72(2), 111-113. https://doi.org/10.1016/j.jpsychores.2011.11.004
McDonald, R. P. (1999). Test theory: A unified treatment. Mahwah. Lawrence Erlbaum Associates, Inc. https://doi.org/10.4324/9781410601087
Muñiz, J., Hernández, A., y Fernández-Hermida, J. (2020). Utilización de los test en España: El Punto de Vista de los Psicólogos. Papeles del Psicólogo, 41(1), 1-15. https://doi.org/10.23923/pap.psicol2020.2921
Murawski, B., Wade, L., Plotnikoff, R., Lubans, D., y Duncan, M. (2018). A systematic review and meta-analysis of cognitive and behavioral interventions to improve sleep health in adults without sleep disorders. Sleep Medicine Reviews, 40, 160-169. https://doi.org/10.1016/j.smrv.2017.12.003
N. Gujarati, D., & C. Porter, D. (2010). Econometría. México, D. F., Mexico: The McGraw-Hill Companies, Inc.
Núñez Bael LN, Vargas Aranda IA, y Aria Zaya LS. (2024). Calidad del sueño en estudiantes de Medicina de la Universidad del Pacifico. Revista científica ciencias de la salad, 6, 01-07. https://doi.org/10.53732/rccsalud/2024.e6303
Perry M. Nicassio, S. R. (2014). Confirmatory Factor Analysis of the Pittsburgh Sleep Quality Index in Rheumatoid Arthritis Patients. Behavioral Sleep Medicine, 12(1), 1-12. https://doi.org/10.1080/15402002.2012.720315
Rebok, F., y Daray, F. M. (2014). Tratamiento integral del insomnio en el adulto mayor. Alcmeon, Revista Argentina de Clínica Neuropsiquiátrica, 18(4), 306-321. https://www.alcmeon.com.ar/18/72/07_rebok.pdf
Royuela Rico, A., y Macías Fernández, J. A. (1997). Propiedades clinimétricas de la versión castellana del cuestionario de Pittsburgh. Vigilia-Sueño, 9(2), 81-94. https://www.researchgate.net/publication/258705863
Royuela Rico, A., Macías Fernández, J. A., y Conde López, V. M. (2000). Calidad de sueño en ancianos. Psiquis, 21(1), 32-39. https://www.researchgate.net/publication/28172011
Sabillón Maldonado, L. N., Peñalva Matute, D. M., y Valle Galo, E. E. (2020). Calidad de sueño y somnolencia diurna en estudiantes de medicina y cirugía de una universidad de San Pedro Sula, Honduras. Revista Médica De La Universidad De Costa Rica, 14(1), 51–60. https://doi.org/10.15517/rmucr.v14i1.42002
Sattler, J. M. (2010). Evaluación infantil; Fundamentos cognitivos. Mexico D. F. El Manual Moderno, S.A. de C.V.
Suardiaz-Muro M, Morante-Ruiz M, Ortega-Moreno M, Ruiz MA, Martín-Plasencia P, y Vela-Bueno A. (2020). Sueño y rendimiento académico en estudiantes universitarios: revisión sistemática. Rev. Neurol, 71 (2), 43-53. doi: 10.33588/rn.7102.2020015
Valverde Jiménez, A., Agüero Sánchez, A. C., y Salazar Mayorga, J. (2020). Manejo del insomnio en el adulto. Revista Ciencia Y Salud Integrando Conocimientos, 4(6), 18–24. https://doi.org/10.34192/cienciaysalud.v4i6.169
Van Breukelen, G., y Vlaeyen, J. (2005). Norming Clinical Questionnaires with Multiple Regression: The Pain Cognition. Psychological Assessment, 17(3), 336-344. https://doi.org/10.1037/1040-3590.17.3.336
Van der Elst, W., Ouwehand, C., van der Werf, G., Kuyper, H., Lee, N., y Jolles, J. (2012). The Amsterdam Executive Function Inventory (AEFI): psychometric properties and demographically corrected normative data for adolescents aged between 15 and 18 years. Journal of Clinical and Experimental Neuropsychology, 34(2), 160-171. https://doi.org/10.1080/13803395.2011.625353
World Medical Association. (2013). World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Journal of the American Medical Association, 310(20), 2191-2194. doi:10.1001/jama.2013.281053